
Oxygen saturation - sO2
Reference interval sO2 - examples Physiological background - sO2 Why measure sO2 ? When should sO2 be measured ? Causes of decreased sO2 Symptoms associated with decreased sO2 Three ways of assessing sO2 in critically ill patients ?
Oxygen saturation (sO2) is the ratio of oxyhemoglobin concentration to concentration of functional hemoglobin (i.e. oxyhemoglobin (O2Hb) and deoxyhemoglobin (HHb) capable of carrying oxygen. Thus [24]:
Bạn đang xem: Oxygen saturation – sO2
The sO2 reflects utilization of the currently available oxygen transport capacity.
In arterial blood 98 - 99 % of oxygenis transported in erythrocytes bound to hemoglobin. The remaining 1 - 2 % of the oxygentransported in blood is dissolved in the blood plasma – this is the portion reported as partial pressure of oxygen (pO2) [6]. (See pO2)
Reference interval sO2 - examples

A sO2 of less than 80 % in adults are regarded as life-threatening [25].
Physiological background - sO2
Each hemoglobin molecule can bind a maximum of four oxygen molecules to form O2Hb (see Hb, O2Hb). The oxygen-delivery function of hemoglobin, i.e. its ability to ”uptake” oxygen in the microvasculature of the lungs, transport it in arterial blood and ”release” it in the microvasculature of the tissue cells, is made possible by a reversible change in the structure of hemoglobin which alters its affinity for oxygen (see Hb) [18]. One significant factor that determines hemoglobin’s affinity for oxygen is the pO2 of the blood. The relationship between pO2 and sO2 is described by the oxyhemoglobin dissociation curve (ODC) (Fig. 5), which reveals in essence that the higher the pO2, the higher is the hemoglobin affinity for oxygen, evident as increasing sO2 [21].
Xem thêm : Tìm hiểu về phản ứng axit axetic và canxi cacbonat
The level of pO2 is highest in arterial blood in the lungs due to the diffusion of inspired oxygen across the alveolar membrane from alveoli to blood (Fig. 3). Consequently hemoglobin has highest affinity for oxygen here, and rapidly binds oxygen becoming almost 100 % saturated – sO2(a) 95-97%. By contrast in the tissues, where pO2 is lower, hemoglobin has decreased affinity for oxygen, resulting in release of oxygen to tissue cells. The sO2 of venous blood (sO2(v)) returning from the tissues to the lungs is consequently decreased (∼75 %) [21]. Illustrated in Fig. 5.
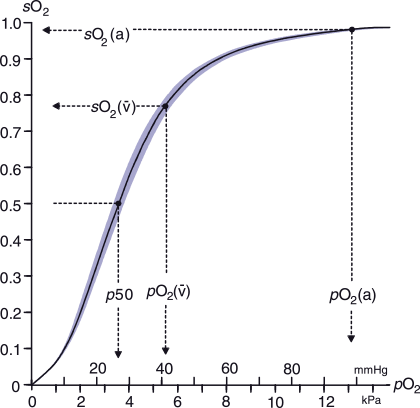
FIG. 5: Oxyhemoglobin dissociation curve.
For more information about the ODC see p50
a: arterial; v: venous
Why measure sO2?
sO2 together with pO2 provides the means for assessing blood oxygenation. Due to the sigmoidal shape of the ODC, sO2 is less informative than pO2, when blood is adequately oxygenated. In the upper flat portion of the curve large changes in pO2 are reflected in much smaller changes in sO2. Indeed, in cases of hyperoxemia (see pO2) sO2 may reach 100 %, and any additional oxygen will only be the oxygen dissolved in blood plasma. Here pO2will remain the only means of assessing blood oxygenation.
sO2 is a major determinant of total oxygen content (see ctO2).
Xem thêm : Fe + H2SO4 → Fe2(SO4)3 + SO2 + H2O
sO2 is a useful parameter for monitoring supplemental-oxygen therapy.
When should sO2 be measured?
Measurement of sO2 is clinically useful in the diagnosis, assessment and monitoring of patients with severe acute or chronic respiratory disease or respiratory failure due to conditions other than respiratory disease (e.g. brain or chest trauma, drug overdose).
Causes leading to impaired sO2 are identical to those for pO2, ctHb or ctO2 (see pO2).
Causes of decreased sO2
Decreased sO2 indicates that oxygen uptake is impaired and may be a result of [14]:
- Mechanical causes (e.g. airway obstruction, chest trauma)
- Neuromuscular diseases (e.g. Guillain-Barré syndrome, myasthenia gravis)
- Drugs that depress the respiratory center (e.g. opioids, heroin, morphine)
- Severe pneumonia
- Pulmonary embolism
- Pulmonary edema
- Acute asthma
- Acute respiratory distress syndrome (ARDS)
- Chronic obstructive pulmonary disease (COPD)
- Pulmonary disease (e.g. fibrosis)
- Pneumothorax
- Cyanotic congenital heart disease
Symptoms associated with decreased sO2
Symptoms associated with hypoxemia and respiratory failure that might prompt sO2 measurement include [14]:
- Breathlessness on minimal exertion
- Shortness of breath/difficulty breathing/respiratory distress (dyspnea)
- Increased respiratory rate (tachypnea)
- Cyanosis
- Nasal flaring
- Wheeze/crackles on auscultation
- Increased sweating (diaphoresis)
- Confusion, disorientation, somnolence
- Coma
- Increased red cell count (polycythemia) with prolonged chronic hypoxemia
Three ways of assessing sO2 in critically ill patients
sO2 can be determined in three ways: Pulse oximetry (SpO2), calculated from pO2, or measured directly on blood gas analyzers. For critically ill patients several studies have demonstrated the importance of using measured sO2 rather than SpO2 or calculated sO2 to avoid mistreatment of these patients [26, 27, 28, 31]. Measured sO2 is preferred in calculations, such as shunt and oxygen content to limit the critically important errors that may result from calculated sO2 [29, 30]. Among intensive-care patients who are at high risk of tissue hypoxia, whether from pulmonary failure, cardiac decompensation, inadequate oxygen transport, or derangements at the cellular level, an accurate measurement of sO2 is essential for planning therapy [32, 33]. The Clinical and Laboratory Standards Institute (CLSI) guideline [24] state with regard to calculated sO2 derived by blood gas analyzers:
“Clinically significant errors can result from incorporation of such an estimated value for sO2 in further calculations such as shunt fraction, or by assuming that the value obtained is equivalent to fractional oxyhemoglobin.”
Nguồn: https://thuvienhaichau.edu.vn
Danh mục: Hóa

